Ignacio Calvo
Reading time:
10
min
Surveillance Gaps, Institutional Erosion and the Epidemiological Cost of Delayed Alerts: The 2026 Bundibugyo Outbreak as a Systemic Case Study
How documented funding cuts to global health surveillance infrastructure produced a measurable detection delay — and why that interval determines the economic trajectory of outbreak response.
Economic evaluation models for infectious disease outbreaks measure with reasonable precision the cost of the response: health expenditure mobilised, international aid committed, GDP loss during the active period of the event. What they measure with far less consistency is the cost of the interval that precedes that response: the window of undetected circulation during which the outbreak accumulates magnitude, geographic dispersal, and containment complexity before any institutional system has formally identified it. That methodological asymmetry is not neutral. It produces a systematic distortion in the evaluation of early warning systems, which tend to be perceived as ordinary operational costs until their absence generates an event that makes them visible.
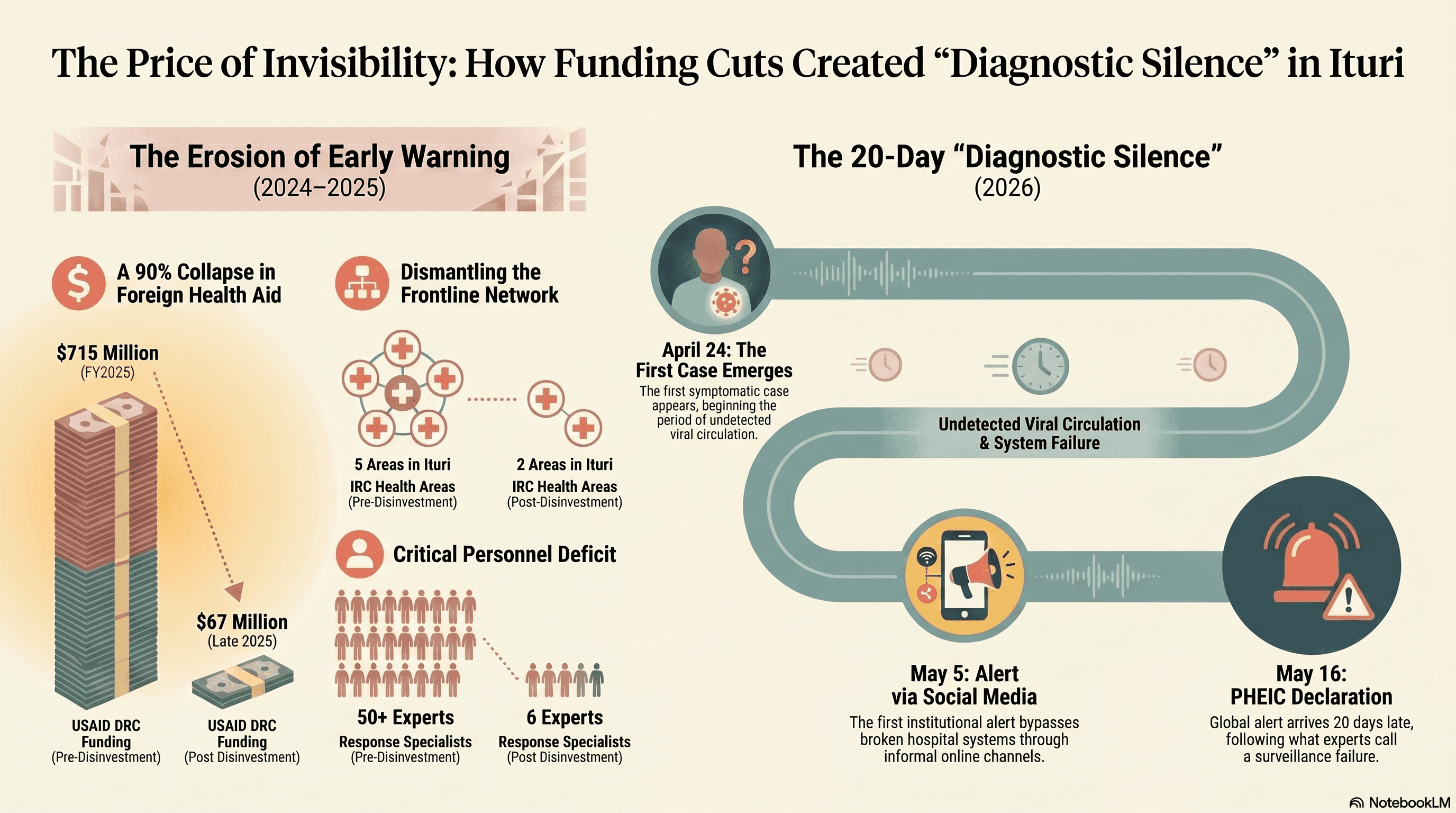
The 2026 Bundibugyo outbreak offers an unusual analytical opportunity to examine that cost with a precision that previous outbreaks rarely allowed. The chronology is documented with verifiable exactness: first symptomatic case on 24 April, first institutional alert on 5 May arriving through social media rather than established hospital systems, first correct diagnostic confirmation on 14 May, PHEIC declaration on 16 May. Twenty days of Diagnostic Silence whose anatomy is reconstructable from primary sources. The head of the DRC's disease surveillance system, Dr. Jean-Jacques Muyembe, was direct in his assessment: "Our surveillance system didn't work." That statement is not a declaration of individual failure. It is the operational diagnosis of a system that arrived at the event without the resources necessary to detect it on time.
The central argument of this analysis is not that cuts to global health funding caused the Ituri outbreak. The argument is more precise and more verifiable: funding cuts reduced the operational capacity of early warning systems in a documented manner, that reduction produced a quantifiable detection delay, and that delay generated a structurally more expensive, more complex, and lower-probability-of-rapid-resolution response than would have been possible with detection two or three weeks earlier. The causal chain is not speculative. It is the sum of disinvestment decisions whose operational consequences the organisations directly involved have documented publicly. The Infrastructure That Disappeared
Understanding the detection failure of the Ituri outbreak requires examining what had ceased to exist in the region before the first symptomatic case appeared. That requires looking at eastern Congo not in May 2026, but twelve months earlier.
USAID sent approximately 67 million dollars in foreign aid to the Democratic Republic of the Congo in the final quarter of 2025, down from 715 million in fiscal year 2025 and nearly 1.2 billion in fiscal year 2024. The majority of that reduction was neither gradual nor planned to minimise operational impact: it resulted from the suspension and cancellation of contracts with non-governmental organisations operating frontline health programmes in the country's most remote regions, including Ituri Province.
Before 2025, US government funding supported a wide range of IRC frontline health and outbreak preparedness activities across eastern DRC, including treatment for communicable and non-communicable diseases, disease surveillance, and the construction and rehabilitation of water, sanitation, and infection prevention and control infrastructure, covering waste management areas, triage zones, handwashing stations, showers, and latrines critical to safely managing infectious disease outbreaks. Much of that funding ended for NGOs in March 2025. As a direct consequence, the IRC was forced to reduce its programming from five health areas in Ituri Province to only two. The three areas eliminated overlap geographically with the epicentre of the current outbreak.
While USAID had previously maintained more than 50 specialists dedicated to outbreak response, cuts left only six people managing simultaneous threats from Ebola, Marburg virus, mpox, and avian influenza. That reduction does not affect only the capacity to respond to an active event. It affects preventive detection capacity, the maintenance of community surveillance networks, and the continuous training of frontline health workers who, in environments like Ituri, constitute the first filter for identifying suspected cases.
Jeremy Konyndyk, former USAID COVID-19 response lead and current president of Refugees International, described the outbreak as the result of a "massive surveillance failure", noting that "it is really unusual for an Ebola outbreak to get to this scale before being detected, particularly in DRC, which has a lot of Ebola experience." The institutional experience accumulated across 17 previous outbreaks is precisely what makes that assessment significant: the system that had learned to detect Ebola earlier than any other country in the world was the one that in 2026 took three weeks to confirm the aetiological agent of an outbreak that had already generated dozens of deaths.
What History Allows Us to Calculate
Assessing the economic risk of the 2026 Bundibugyo outbreak does not require original projections or speculative modelling. The available literature provides a sufficiently robust reference base to situate the potential cost within a comprehensible scale, and to establish which variable determines at which point on that scale the final event will be positioned.
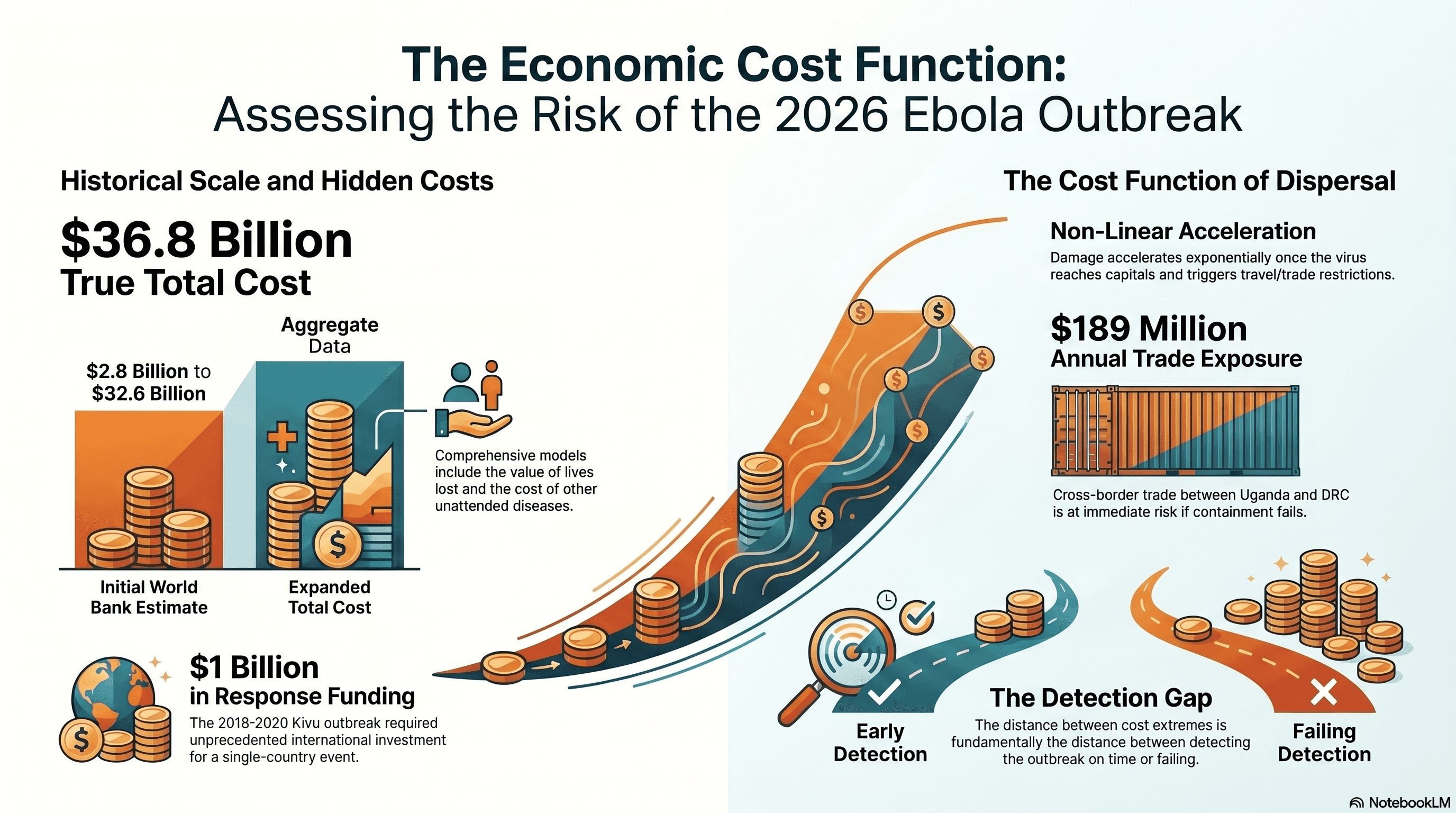
World Bank estimates established that the 2014-2016 West Africa outbreak generated losses of between 2.8 and 32.6 billion dollars depending on the propagation scenario considered, with the most severe impact concentrated in Guinea, Liberia, and Sierra Leone, where GDP growth fell between 2.3 and 11.7 percentage points. That range does not reflect methodological uncertainty: it reflects the operational difference between a scenario of early containment and a scenario of regional dispersal. The distance between both extremes of the estimate is, fundamentally, the distance between detecting the outbreak on time and failing to do so.
A subsequent analysis published in the Journal of Infectious Diseases (Oxford) expanded that estimate by including components that World Bank models had excluded: the economic value of lives lost, the cost of affected health workers, and the impact of non-Ebola diseases left unattended during the outbreak, reaching a total cost estimate of 36.8 billion dollars. The difference between that figure and the initial estimates reflects a principle that response models rarely incorporate with sufficient weight: when a health system mobilises all its resources toward a single event, the cost of the rest of the care it ceases to provide does not disappear. It accumulates.
The Kivu outbreak of 2018-2020, geographically and contextually the closest precedent to Ituri 2026, received more than 1 billion dollars in international response funding over 26 months, constituting the highest investment in control of a single-country Ebola outbreak in documented history. That level of mobilisation was possible because the international community still had the institutional and financial infrastructure to sustain it. In 2026, part of that infrastructure no longer exists under the same conditions.
What these data establish is not a quantitative forecast for the current outbreak, but a cost function with known properties. The economic magnitude of the damage does not grow linearly with case numbers. It accelerates as the outbreak surpasses local containment thresholds, reaches capitals with international connectivity, and generates travel restrictions that paralyse regional trade. Uganda exports approximately 189 million dollars annually in goods to the DRC, illustrating the scale of cross-border commercial exchange exposed when an outbreak crosses that border without having been contained. The border measures that followed confirmation of cases in Kampala carry consequences not only for health operations, but for supply chains, food security, and the economic mobility of populations already functioning under conditions of extreme fragility. The Interval That Determines the Curve
The operational paradox of the Ituri outbreak is that the twenty days of Diagnostic Silence between the first symptomatic case and the first institutional alert did not produce exclusively epidemiological damage. They produced a shift on the cost curve with structural consequences for the type of response that became necessary.
By 5 May, when the first notification reached the WHO, the ring containment strategy that had proven effective in previous DRC outbreaks was no longer applicable in its conventional form. Cases had migrated from Mongbwalu through the Ituri health network to Bunia, and from there into Uganda, before any isolation protocol was active. The IRC warned that the increase in suspected cases from 246 to more than 500 in just 96 hours reflected the reality that surveillance systems were catching up with transmission that had likely been occurring for some time. That technically precise formulation describes something operationally concrete: the response activated in May 2026 was not a containment response. It was active dispersal management, a response category with a considerably higher cost per case managed than early containment, and a significantly longer resolution horizon.
That converts the cost of surveillance disinvestment into something calculable in relative terms, even without definitive economic projections for the current outbreak. Each week of Diagnostic Silence does not only expand the number of cases the response must manage. It advances the moment at which the outbreak exceeds the threshold of local management and requires international resource mobilisation, with all the logistical, coordinative, and political costs that implies. The disinvestment in early warning systems did not produce only a larger outbreak. It produced the need for a structurally more expensive response, sustained over a longer period, on a more complex epidemiological terrain than would have existed with two or three fewer weeks of undetected circulation.
The cost function that historical literature describes is not, in this sense, a theoretical abstraction. It is the framework within which surveillance infrastructure funding decisions can be evaluated with the same logic applied to any other risk prevention investment: the cost of maintaining the system active versus the cost of activating the response after the system has failed. Data from previous outbreaks establishes consistently that the second option is between five and ten times more expensive than the first, and that relationship holds independently of the biological agent involved. Surveillance as Infrastructure, Not Expenditure
The 2026 Bundibugyo outbreak does not introduce a new idea into the global public health debate. It introduces empirical demonstration of a principle that epidemiological literature has been formulating since at least the West Africa outbreak: disease surveillance systems are cost-efficiency infrastructure, not discretionary expenditure subject to political cycles. What distinguishes the 2026 outbreak from previous theoretical formulations is that the causal chain between disinvestment, detection failure, and escalating response cost is documented with unusual precision, from funding reduction figures to the number of eliminated programme areas, from the date of the cuts to the date of the first undetected case.
The WHO representative in the DRC, Anne Ancia, stated on 19 May that funding reductions had had a "tremendous impact" on the country's capacity to combat Ebola. Africa CDC, for its part, acknowledged that the true index case of the outbreak remains unknown, meaning the virus circulated for a period whose total duration cannot yet be established with precision. That chronological uncertainty about the most severe event recorded in the region is not a minor data point: it is the operational reflection of a surveillance system that was reduced below the functional threshold necessary to generate the epidemiological traceability the response required from the outset.
The implication of this analysis does not require taking a position in political debates about foreign aid funding, which have dimensions that exceed operational epidemiological analysis. It requires recognising, with the available data, that early warning infrastructure is not interchangeable with other categories of global health public expenditure. It is the variable that determines at which point on the cost curve the outbreak response activates. And that variable, unlike the biology of the pathogen or the geography of the epicentre, is entirely modifiable through sustained health policy decisions and institutional investment.
In Ituri, in May 2026, that variable arrived at the event in conditions of structural fragility. The result is the third Ebola PHEIC in the history of the International Health Regulations, the first caused by the Bundibugyo strain, and the first declared without prior convening of the Emergency Committee because the speed of deterioration left no time for standard procedures. Those three simultaneous facts are not coincidence. They are the accumulated consequence of a system that was weakened before the event it was supposed to detect appeared.
References: 1. IRC. "Funding cuts led to delayed detection of deadly Ebola outbreak in DRC." Press release, 19 May 2026. https://www.rescue.org/press-release/funding-cuts-led-delayed-detection-ebola-outbreak-drc 2. STAT News. "Trump's cuts to foreign aid are undermining the Ebola response, insiders say." 19 May 2026. https://www.statnews.com/2026/05/19/us-aid-cuts-hamper-drc-ebola-response/ 3. Common Dreams. "Public Health Experts Point to Trump Aid Cuts as WHO Declares Emergency Over Ebola Outbreak in DRC, Uganda." 18 May 2026. https://www.commondreams.org/news/ebola-drc-congo 4. NPR. "WHO chief concerned over 'scale and speed' of Ebola outbreak." 20 May 2026. https://www.npr.org/2026/05/20/g-s1-122971/who-chief-concerned-over-scale-and-speed-of-ebola-outbreak 5. WHO. "Ebola disease caused by Bundibugyo virus, DRC and Uganda." DON602. 16 May 2026. https://www.who.int/emergencies/disease-outbreak-news/item/2026-DON602 6. WHO. "Epidemic of Ebola Disease determined a PHEIC." 17 May 2026. https://www.who.int/news/item/17-05-2026 7. Africa CDC. "Africa CDC Declares Bundibugyo Ebola Outbreak a Public Health Emergency of Continental Security." 18 May 2026. https://africacdc.org
8. World Bank. "The Economic Impact of the 2014 Ebola Epidemic: Short and Medium Term Estimates for West Africa." October 2014.
9. Pratt B, et al. "Economic and Social Burden of the 2014 Ebola Outbreak in West Africa." Journal of Infectious Diseases. 2018;218(Suppl 5):S698–S706. DOI: 10.1093/infdis/jiy213
10. Colombini A, et al. "The cost of public health interventions to respond to the 10th Ebola outbreak in the Democratic Republic of the Congo." PLOS ONE / PubMed. 2023. PMID: 37848269
11. Al Jazeera. "Ebola tests resilience of Uganda's cross-border trade." 2019. https://www.aljazeera.com/economy/2019/10/11/ebola-tests-resilience-of-ugandas-cross-border-trade